Huge Toronto condo tower planned for over a decade might finally happen
Plans to tear down a midtown Toronto office building and construct a soaring condo tower have been in the works for a decade now, and a new plan filed with the City last month could finally result in big changes just east of the Yonge and Eglinton intersection.
Developer State Building Group has long been eyeing its property at 55 Eglinton Avenue East as a redevelopment cash cow. Currently home to an eight-storey office building, the owners have been planning to level the mid-rise property and replace it with a high-rise that would keep in character with the changing face of this artery.
The project was first proposed as a 47-storey mixed-use tower back in the closing days of 2014, and almost exactly one decade and several revisions later, it is now inching closer to realization with a planned height of 55 storeys.

The City refused that early plan, citing its elimination of employment space in favour of residential. This led to a revisions tabled a few years later that retained office space and increased the overall height to 50 storeys.
The 50-storey plan was eventually granted approval by the Ontario Land Tribunal in 2017, but aside from some resubmissions that made some minor changes, activity has mostly fallen silent in the years since. At least, that was the case until December 2024, when updated plans were filed for the site that sought to pack on even more density.
An early December application for the site now seeks Official Plan and zoning by-law amendments to permit a 55-storey tower at 55 Eglinton East, a five-storey increase over the approved plan.

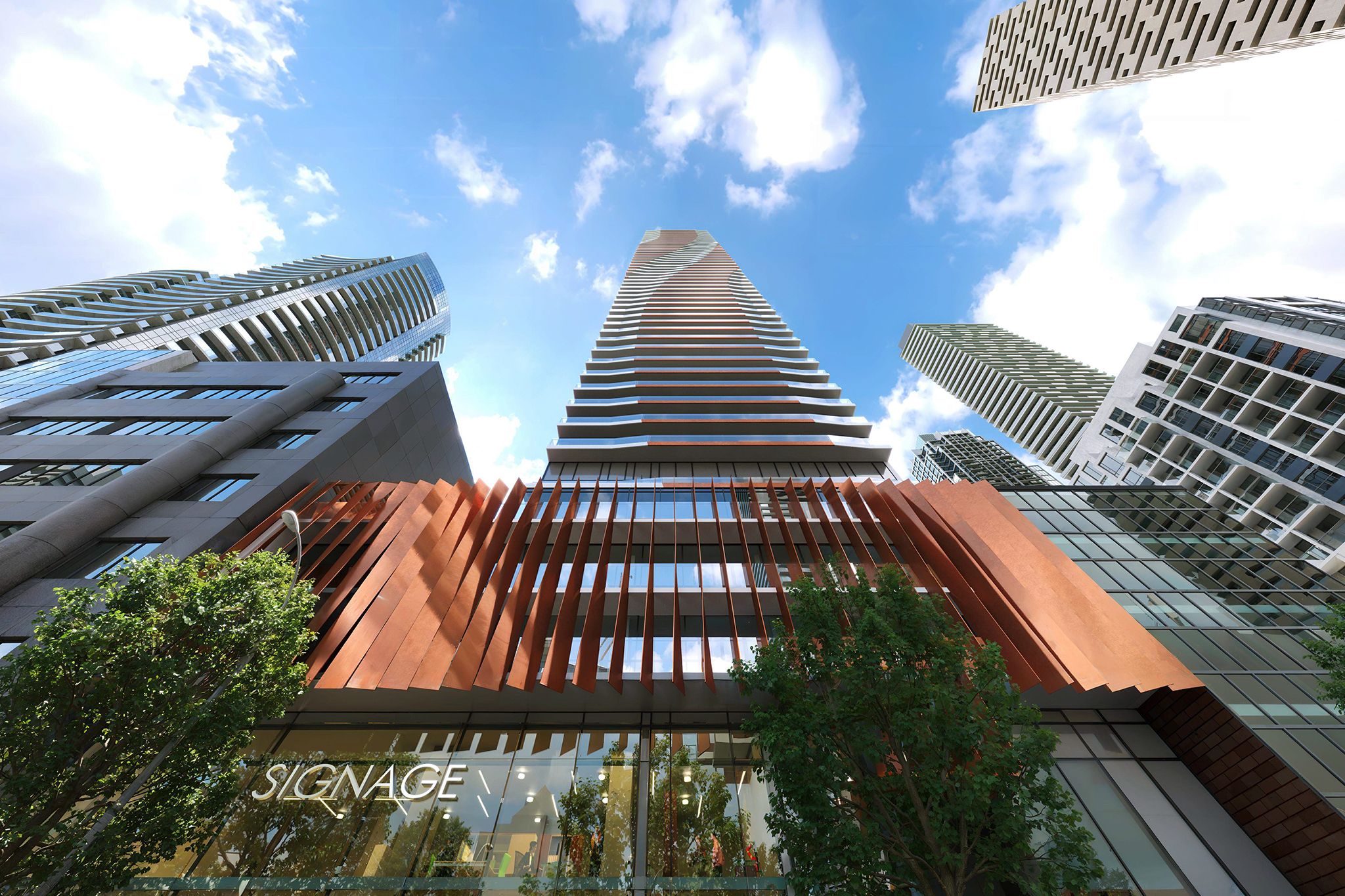
As with previous versions, the project features a design from KIRKOR Architects that boasts vibrant flashes of orange bookending the tower with sections at street level and framing the roofline.
The revised plan would rise to a height of over 180 metres, and would join a growing corridor of similarly-scaled high-rises lining the central stretch of the forthcoming Eglinton Crosstown LRT.
One key change in the updated proposal is the removal of office replacement space.
While the loss of office space was a key point of contention between the City and developer during the early planning process, the commercial market has faced major challenges in the years since, leading the City to axe its office space replacement requirements for redevelopment projects.
The increase in storeys and slashing of commercial space has resulted in a higher unit count than earlier versions of the plan. A total of 664 residential units are proposed in the late 2024 plan, up from 461 in the previous 50-storey version and 455 in the initial 2014 submission.

Another change introduced courtesy of the removal of office space is a mix of over 300 square metres of street-fronting retail space along with a minimum of seven affordable housing units within a combined 644-square-metre area of the building.
Despite the City's relaxation of office replacement requirements, an Official Plan Amendment application was required for this submission seeking to exempt the development from a policy in the Yonge-Eglinton Secondary Plan, which would require the full replacement of existing office space.
Kirkor Architects
Latest Videos
Latest Videos
Join the conversation Load comments







