
Air Canada and WestJet just ranked among the worst airlines for cancellations
According to a new ranking, Air Canada and WestJet are among the top 10 airlines in North America with the most cancelled flights.
Cirium, which provides aviation analytics, has released its 2024 on-time performance review of airlines and airports worldwide.
It's been quite the year for the aviation industry with weather anomalies and a CrowdStrike outage.
Jeremy Bowen, CEO of Cirium, said, "Despite these hurdles, airlines and airports continued to prioritize operational excellence, achieving impressive levels of reliability and passenger satisfaction."
The survey reveals the airlines with the highest number of cancellations by region. In North America, the list is dominated by US carriers, with American Airlines taking first place with the highest number of cancelled flights. In 2024, 2,177,418 American Airlines flights took off, while 28,649 flights were cancelled.
Air Canada comes in fourth place with 386,082 scheduled flights that took off. However, it also cancelled 10,816 flights. Alberta-based low-cost carrier WestJet came in seventh in North America — last year, it had 192,323 flights, and 6,131 were cancelled flights. 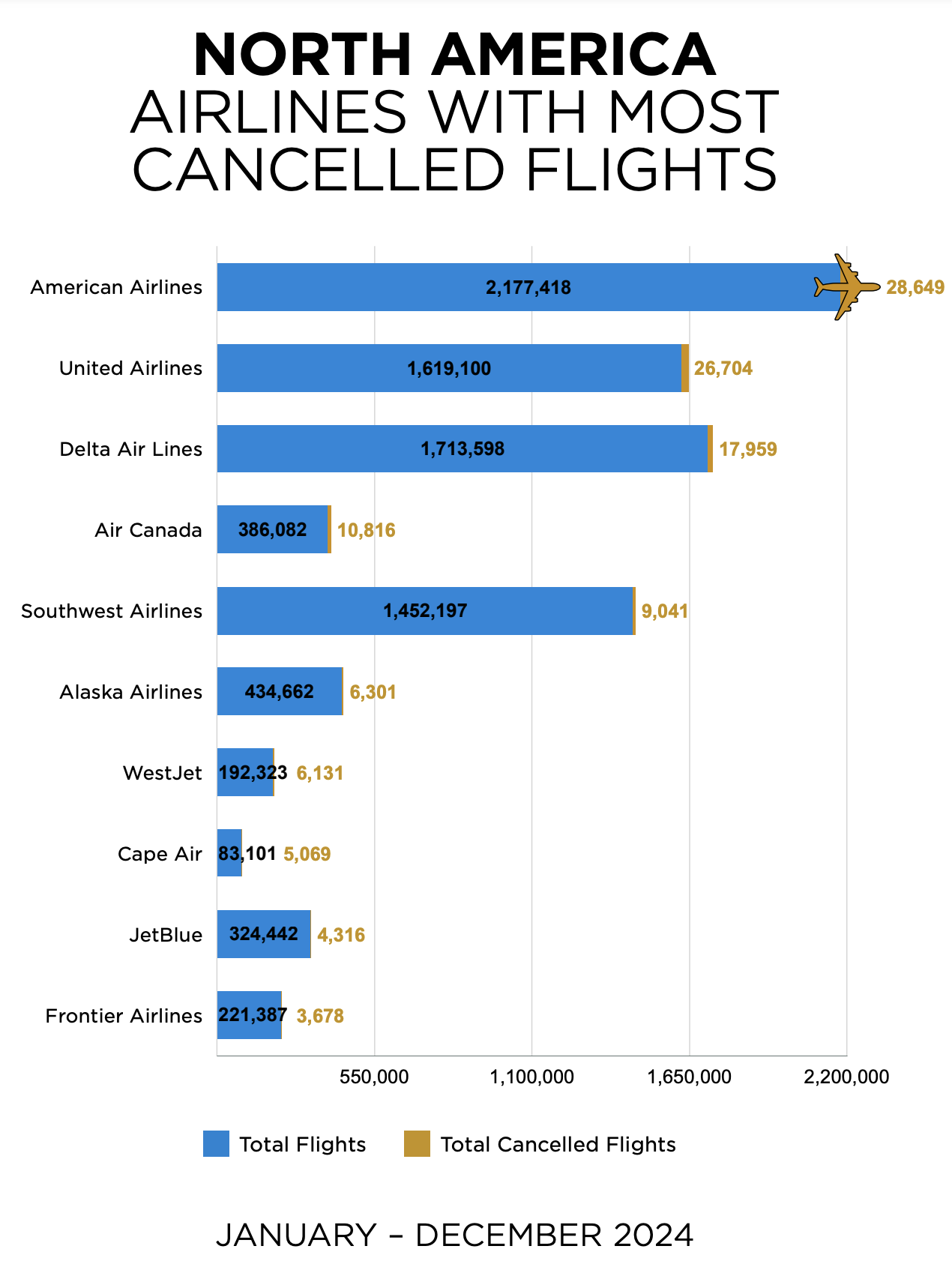 Globally, North America had the second-highest number of cancelled flights — 9,925,300 scheduled flights and a total of 135,744 cancellations. That's just behind airlines in the Asia Pacific, which saw 12,489,263 flights and a staggering 315,317 cancellations.
Globally, North America had the second-highest number of cancelled flights — 9,925,300 scheduled flights and a total of 135,744 cancellations. That's just behind airlines in the Asia Pacific, which saw 12,489,263 flights and a staggering 315,317 cancellations.
Despite making the top 10 for cancelled flights, Air Canada and WestJet are among the top 10 airlines in North America that got passengers to their destinations on time.
Air Canada takes the ninth spot for on-time arrivals — out of 385,703 flights, 71.36 per cent arrived on time. Just behind Air Canada in the 10th place is WestJet. In 2024, the airline had a total of 192,084 flights, 70.99 per cent of which arrived as scheduled. 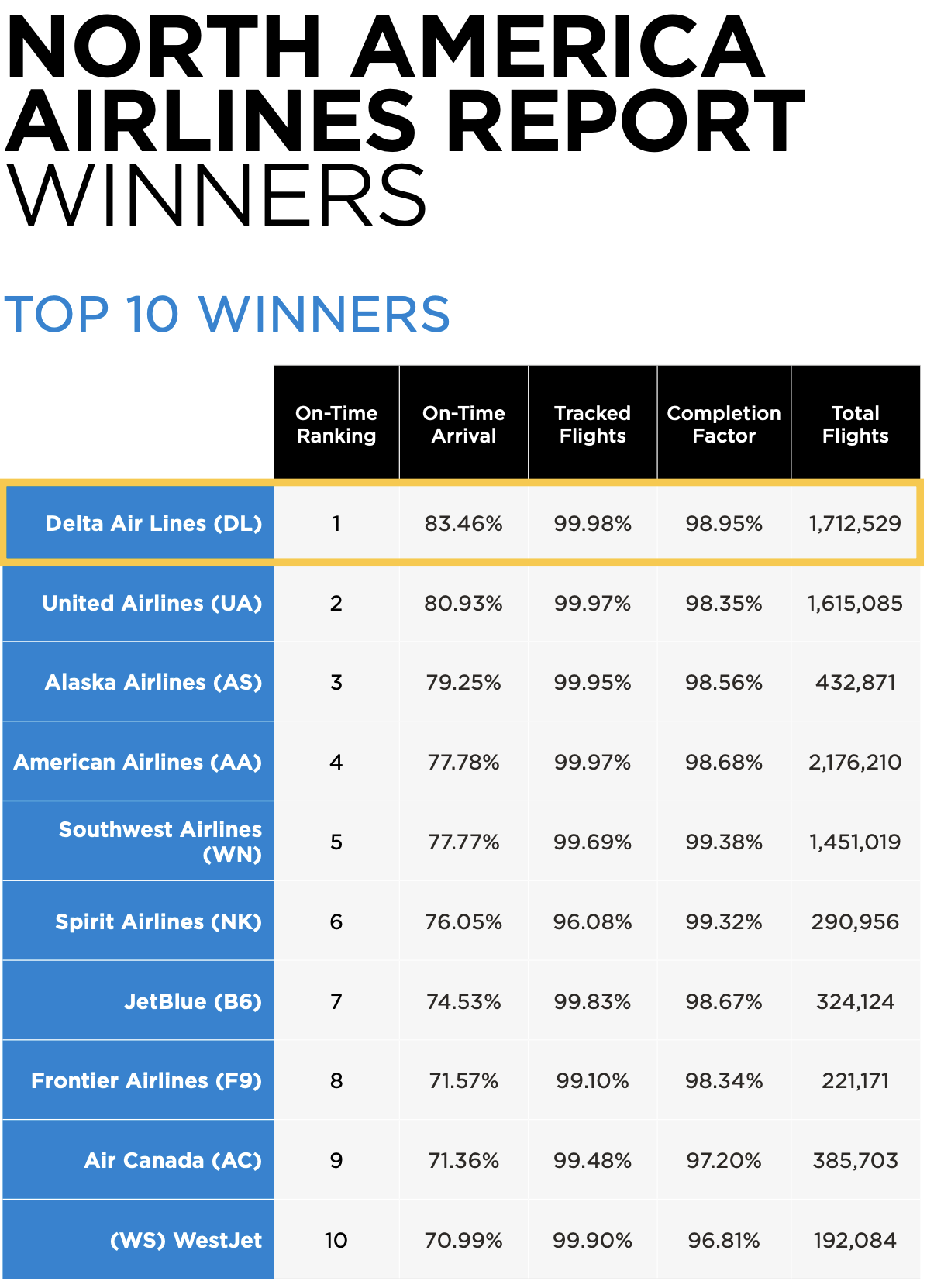 According to the report, Saudi Arabia's Riyadh King Khalid International Airport was the top airport globally with the best on-time performance. The airport serves 60 airlines and had 86.65 per cent on-time departures and 81.79 per cent on-time arrivals.
According to the report, Saudi Arabia's Riyadh King Khalid International Airport was the top airport globally with the best on-time performance. The airport serves 60 airlines and had 86.65 per cent on-time departures and 81.79 per cent on-time arrivals.
Not one Canadian airport made the top 20 list.
Latest Videos
Latest Videos
Join the conversation Load comments







